The Whitecoat Rebellion
The Rebellion Is Real.
500 White Coats Already Marched.
The outrage you felt watching physicians fight back — it materialized. On May 21, 2026, 500 doctors, nurses, and healthcare workers marched on Capitol Hill. Dr. Potter sat in private Congressional meetings the day before. FIGS organized it, funded it, and co-wrote the legislation. Noah Wyle brought the cameras and his mother, a nurse of 50 years.
The rebellion doesn't need you to start something. It needs you to plug into something already moving. This is the patient side — the documented case for why physicians are marching, and what to do if you're a physician, patient, journalist, or legislator who wants in.
The Rebellion That Materialized
Healthcare is Human — Capitol Hill, May 21, 2026
How We Got Here
"The Whitecoat Rebellion" written in direct response to Dr. Potter's call. The song named what was coming.
FIGS and actor Noah Wyle (The Pitt / ER) announce a formal long-term advocacy partnership focused on healthcare workforce and medical debt.
Dr. Potter + Noah Wyle hold private bipartisan Congressional meetings — one day before the public rally.
500 white coats march on Upper Senate Park. Bernie Sanders, Tim Kaine, and bipartisan House members show. The song was right.
Bills on the Table
Healthcare is Human Act
Up to $6,000/year tax credit for healthcare workers in shortage areas. FIGS co-wrote this bill. Bipartisan sponsors.
Dr. Lorna Breen Healthcare Provider Protection Act
Funds mental health programs for healthcare workers pushed to breaking point by the system.
Speak FREE Act
Federal whistleblower protection for workers who report safety concerns — the cease-and-desist protection Dr. Potter never had.
The Anthem
The Whitecoat Rebellion
Written January 18, 2026 — a direct response to Dr. Potter's call. "Calling every physician with a camera and spine — record the institutional malpractice, post it online." The movement has a song. This page is where the song becomes action.
Who are you?
🩺 For Physicians & Clinicians
You already know. Every peer-to-peer call where the reviewer can't name the specialty. Every appeal that gets overturned in minutes. Every patient who waited months for care you ordered on day one. Here is what to do with what you know.
Name the legislation publicly.
Two bills. Both names matter. Every time you make content about prior authorizationPrior AuthorizationA health-insurance process that requires your doctor to get advance approval from your plan before it will cover a specific service, procedure, or drug. abuse, name them. Not "proposed legislation." Not "reform efforts." The names.
S.3829
Corporate Crimes Against Healthcare Act
Criminal penalties for executives. Unjust enrichment clawbacks. Sponsored by Sen. Elizabeth Warren.
S.3822
Break Up Big Medicine Act
Forces divestiture of insurer + physician group + PBM vertical integration. Bipartisan: Warren + Hawley.
Rep. Neal Dunn, MD (R-FL) — a urologic surgeon — said from the House floor that prior authorization is the practice of medicine and insurers should pay malpractice insurance too. The Republican floor support is there. Use it.
Use this documentation. You have explicit permission.
Everything on this site is documented, cited, and sourced. The IRE overturn rates. The recorded phone calls. The deposition transcripts. The FDAFDAThe U.S. Food and Drug Administration (FDA) decides whether drugs, biologics, and medical devices are safe and effective enough to be sold. clinical trial data. The physician who copied a nurse's note and typed "agree." The pediatrician overriding a board-certified bariatric specialist.
Link back or don't — the data matters more than the credit. If you want to verify before you cite, the primary sources are in the Problem Room and the full PSI briefing is available as a PDF.
Document your peer-to-peer calls.
With patient consent, document everything the reviewing physician says — and everything they don't. Their name if they'll give it. Their specialty. What objective clinical data they refused to consider and why. Whether they'd treated a patient like yours in the last year.
Dr. Elisabeth Potter recorded a peer-to-peer call and discovered the reviewer was an ocular plastic surgeon overriding a lymphedema surgery for a breast cancer patient. UHC demanded she apologize publicly and take the video down. She refused. That documentation is now evidence of exactly the mechanism the Clinical Integrity Amendment was written to stop.
Under the Clinical Integrity Amendment § 2: a reviewing physician who is not board-certified in the same or directly relevant specialty as the treating physician has no valid authority to issue the denial. Every documented case of specialty mismatch is evidence for why this provision must exist in federal law.
Tell your patients they can appeal — and give them the number.
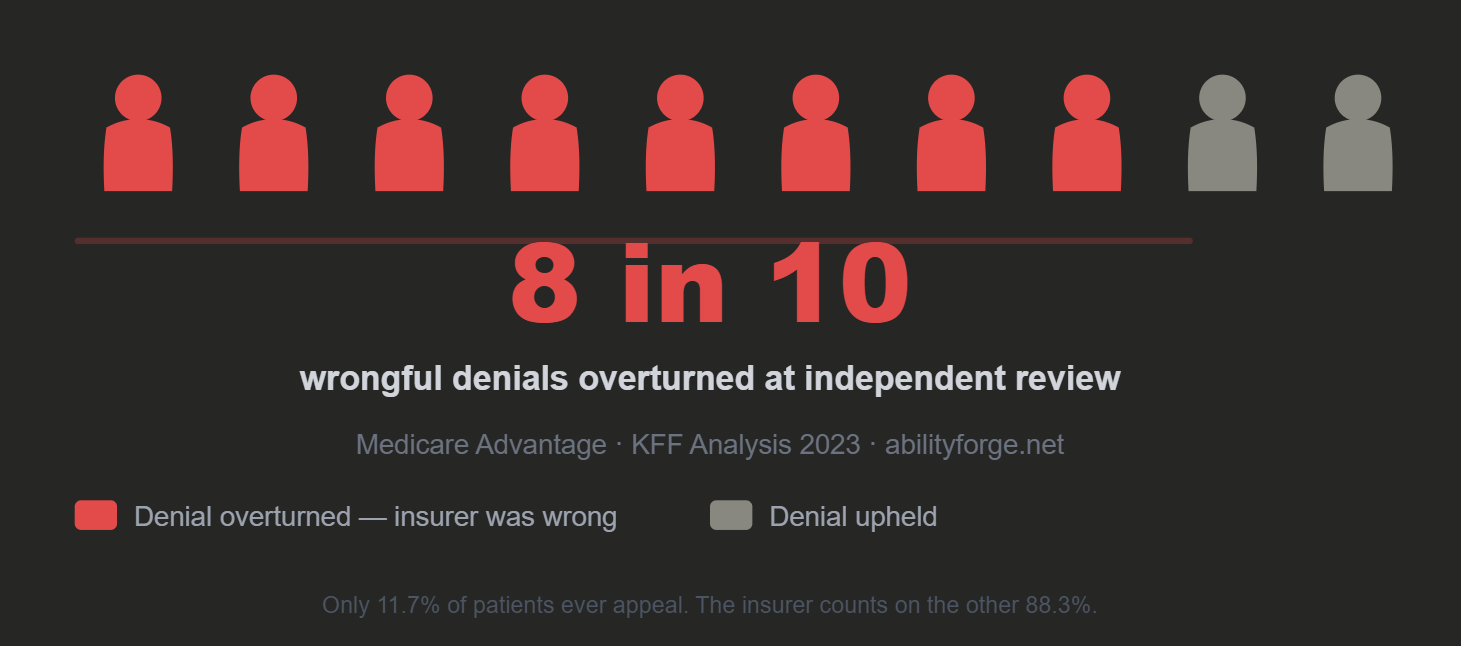
81.7% of appealed Medicare Advantage denials are overturned at Independent Review. Only 11.7% of patients ever appeal. Your patients don't know this. The insurer is counting on that.
81.7%
of appealed denials overturned
11.7%
of patients ever appeal
0.2%
of MA patients appeal — what UHC counts on
For every 1,000 denials CenteneCenteneThe dominant Medicaid managed care organization in the United States, operating in most states. Also a major ACA marketplace insurer. issues, approximately 2 patients appeal, and 998 accept a denial an independent physician would overturn 93.6% of the time. — KFFKFFKFF (formerly the Kaiser Family Foundation) is an independent, nonpartisan source of health-policy research, polling, and journalism. 2023
If you have been the one signing denials under corporate pressure — we are not your enemy.
Dr. Cates, the UHC reviewer deposed in the McNaughton case, testified under oath that he did approximately 100 reviews per week, had not treated ulcerative colitis patients in his own practice, and copied a nurse's note and typed "agree." UHC's policies explicitly prevented him from considering that the patient had failed every prior treatment.
The Clinical Integrity Amendment is not designed to punish physicians trapped in a system that weaponizes their licenses. It is designed to dismantle the system that puts them there — by making the corporate structure behind the denial personally, professionally, and legally accountable. If you have a story from inside that system, we want to hear it.
Independent Voices — Full Record
Six physicians. One convergent diagnosis. →
Dr. Glaucomflecken · Dr. Elisabeth Potter · Dr. Caleb Masterson · Dr. J Mack Slaughter Jr · DocSchmidt · Dr. Ibrar — the documented case that prior authorization is the practice of medicine, made from every direction simultaneously.
🙋 For Patients & Advocates
They are counting on you not fighting back. The numbers prove it. Here is what they don't want you to know — and what to do with it.
You have the right to appeal. Exercise it. The odds are in your favor.
81.7% of appealed Medicare Advantage denials are overturned by an independent physician reviewer. That reviewer has no financial stake in the outcome. The insurer denied you anyway — because they calculated that you wouldn't fight back. When you appeal, you win most of the time. When you don't appeal, they win every time.
For Medicare Advantage denials:
Request a Qualified Independent Contractor (QIC) review or an Independent Review Entity (IRE) review. You do not need a lawyer. You need the denial letter, your medical records, and a letter from your treating physician explaining why the treatment is medically necessary.
Ask for the peer-to-peer. Ask for the reviewer's name and specialty in writing.
Your doctor has the right to speak directly to the reviewing physician. Request this in writing and ask your physician to initiate it. When the call happens, ask your physician to document the reviewer's specialty and what clinical data they refused to consider — and why.
In documented cases, UHC reviewers have refused to provide their name citing "personal safety." A pediatrician overrode a board-certified bariatric specialist for an adult patient. An ocular plastic surgeon overrode a lymphedema surgeon for a breast cancer patient. These are not rare. They are documented instances of a pattern. Documenting yours adds to the evidence.
Contact your senators. Both of them. Today.
Two bills. Tell them you want a co-sponsor. Tell them prior authorization killed someone you know, nearly killed someone you love, or is happening to you right now. Personal testimony from constituents moves legislation. A form letter doesn't. A phone call does.
S.3829
Corporate Crimes Against Healthcare Act
Criminal accountability for executives whose decisions harm patients.
S.3822
Break Up Big Medicine Act
Forces the breakup of the insurer-PBM-physician conglomerate. Warren + Hawley. Bipartisan.
Share your story. Your case is evidence.
Every documented case of wrongful denial that includes a denial letter, a reviewer specialty mismatch, a shifting rationale, or an IRE overturn is a data point in a provable pattern of systemic fraud. The Wrongful Denial Echo Chamber operates on the assumption that isolated cases stay isolated. They don't when they're documented together.
Share Your Story →📰 For Journalists & Researchers
The documentation is complete. Primary sources are public and linked. The PSI briefing, the clinical trial data, the deposition excerpts, the IRE overturn documentation — all of it is available without a records request.
Primary Source Documents
Senate PSI Briefing
Prior Knowledge OmissionPrior Knowledge OmissionA denial issued without referencing documented clinical evidence already present in the patient's medical record that establishes medical necessity. — Documented Fraud Mechanism
Submitted to the Senate Permanent Subcommittee on Investigations, March 2026. Timestamped paper trail, physician corroboration, IRE overturn as evidentiary foundation.
Download PDF →Executive Summary
Scoped to liability elements: scienter, material misrepresentation, Prior Knowledge Omission. Damages and causation chain documented.
Download PDF →Medicare Coverage Rule
LCD L33787LCD L33787A Local Coverage Determination issued by Medicare Administrative Contractors governing skin substitute coverage — including Apligraf. — Lower Limb Prostheses
The Medicare coverage determination UHC violated. K3 qualifying criteria documented. All three criteria met. Denial issued anyway.
K-Levels — the Medicare functional classification system (K0–K4) that determines prosthetic eligibility. Learn more →
Download PDF →FDA Regulatory Record
ApligrafApligrafAn FDA-approved living cell therapy and bioengineered skin substitute used in chronic wound care, including diabetic foot ulcers and venous leg ulcers.® — Summary of Safety & Effectiveness
PMA P950032. Approved 1998 and 2000. Reduces amputation risk 60%, osteomyelitis risk 75%. Denied for 17 months as "not medically necessary."
Download PDF →Legislative Text
Clinical Integrity & Patient Safety Amendment
Proposed addition to S.3829. Five sections. Specialty matching, Prior Knowledge Omission prohibition, Buffer Fund, malpractice trigger.
Download PDF →Legal Framework
Denial on Trial — Medical Due Process
Applies Gideon v. WainwrightGideon v. Wainwright1963 U.S. Supreme Court ruling establishing that the Sixth Amendment guarantees the right to appointed counsel for defendants who cannot afford an attorney. logic to the IRE system. Burden of proof. Administrative Law Judge model. Proposed federal architecture.
Download PDF →Published Coverage of This Case
Press inquiries and document requests:
All documentation on this site is public and available without embargo. For additional primary sources, physician contacts willing to speak on record, or case-specific inquiries, use the contact form at abilityforge.net/contact. Responses within 24 hours.
🏛️ For Legislators & Staff
The legislative architecture is complete and bipartisan. The documented case with a timestamped paper trail has been submitted to the Senate Permanent Subcommittee on Investigations. The Republican floor validation exists. Here is the full picture.
The Bipartisan Architecture
S.3822
Break Up Big Medicine Act
Warren (D-MA) + Hawley (R-MO)
One of the most politically unlikely alliances in recent healthcare legislation, united by what the bill calls "an unprecedented wave of consolidation."
S.3829
Corporate Crimes Against Healthcare Act
Warren, Blumenthal, Markey, Merkley, Welch
Criminal penalties and executive clawbacks. Open to additional co-sponsors.
Floor Validation
Rep. Neal Dunn, MD (R-FL)
Urologic surgeon. House hearing on healthcare affordability.
"Prior authorization is the practice of medicine. And I would invite them into the medical liability arena."
The gap in the current architecture:
S.3829 reaches the corporation and its executive leadership. It does not reach the individual physician who signs the denial letter. The Clinical Integrity Amendment closes this gap by attaching personal professional accountability — mandatory State Medical Board referral — to every IRE overturn that documents a specialty mismatch or Prior Knowledge Omission. Rep. Dunn's floor statement is the legal foundation that makes this coherent: you cannot claim immunity for a decision that is, by the admission of a physician-congressman, the practice of medicine.
The Documented Mechanism — Prior Knowledge Omission
The PSI submission documents a specific, repeatable, and prosecutable fraud pattern: an insurer acknowledges a patient's qualifying status through an approval decision, then denies a directly related claim while possessing that prior knowledge. The Maximus IRE overturn on October 2, 2023 — issued within days of the denial — is the equivalent of summary judgment: UHC's position was indefensible. This is not a medical disagreement rate. It is a business model.
The cascading taxpayer cost — one case:
A denied $55,000 procedure (iliac vein stenting, 85–90% five-year patency rate) → 17-month delay in FDA-approved wound care → osteomyelitis → above-knee amputation → ongoing prosthetic, wound care, surgical, and rehabilitation costs. Total taxpayer-funded cost: $1.1 million and climbing. The insurer paid nothing. The patient paid with his limb. The public paid with their taxes.
📋 The Citable Fact Kit
Pull-ready statistics for content creators. Every number is sourced. Click the source link to verify before you cite.
IRE Overturn Rates — KFF 2023
These numbers share a specific meaning: a physician with no financial stake in the outcome reviewed the denial and said the insurer was wrong — between 81.7% and 93.6% of the time.
 Source: KFF Analysis →
Source: KFF Analysis →
The Appeal Gap
49.8M
Prior authorization requests to Medicare Advantage insurers in 2023 — up from 37M in 2021
3.7M
Denials issued. Only 11.7% of those were ever appealed.
0.2%
Of Medicare Advantage policyholders appeal any denial. The business model depends on this number staying low.
AI as Weapon — nH Predict
~90%
Alleged error rate of UHC's nH Predict AI algorithm. Deployed across Medicare Advantage to automate post-acute care denials. Used anyway.
9x
Increase in UHC skilled nursing facility denial rate from 2019 (1.4%) to 2022 (12.6%) — coinciding directly with nH Predict deployment
The baseline it replaced:
UHC's own human reviewers were overturned 85.2% of the time in 2023. The algorithm scripted to replace them was wrong 90% of the time. You don't accidentally build something worse than your own baseline.
The Cost of One Denial
$55K
Denied iliac vein stenting procedure
$1.1M+
Taxpayer-funded costs that followed
17 months → 2 weeks
FDA-approved Apligraf denied for 17 months. When finally approved, it closed the wounds in two weeks. Bone demineralization described as "cuttable with a scalpel" had occurred in between.
The Wrongful Denial Echo Chamber does not save money. It shifts costs from the insurer onto taxpayers and onto the patient's body.
The White Coat Rebellion — Scale
40+
Health systems dropping Medicare Advantage plans — nationally
60K
Patients displaced when Johns HopkinsJohns HopkinsA research university and hospital system in Baltimore, Maryland. One of the most cited medical research institutions in the world. left UHC's network — not over money, over denials
~90K
Physicians now employed by UHG's Optum — the largest physician employer in the U.S.
80%
Of all U.S. doctors now employed by corporate entities. More than three in four.
🎙️
An Open Invitation
Doing this work? There's a place for you here.
AbilityForge builds pages for the people fighting the wrongful-denial machine — and the people living it. If you're a physician, nurse, patient, advocate, or lawmaker with a story, a tool, or a fight worth documenting, we'll build you a home for it. No cost. No catch.
Get featured
Have your work, your case, or your campaign documented here — the way Dr. Ibrar, Anna Harris, and Jessica Baladad are. Your voice, your consent, your call on how it's framed.
Use the whole site — free
Every stat, source, chart, and document here is a free resource for your own content. Pull what you need for your posts, videos, testimony, or reporting. Link back or don't — the data matters more than the credit.
Tell me who you are and what you're fighting. We'll take it from there.